CLINICAL,FORENSIC,AND ETHICS CONSULTATION IN MENTAL HEALTH
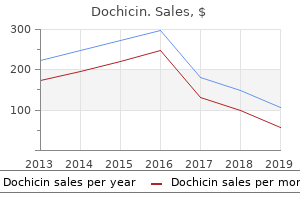
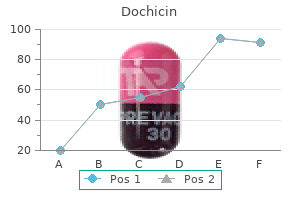
Dochicin
"Buy dochicin 0.5mg online, virus and trip".
By: Q. Nefarius, M.B.A., M.D.
Assistant Professor, Louisiana State University School of Medicine in Shreveport
Success charges are restricted when solely endocardial mapping and ablation strategies are used antibiotics pharmacology discount 0.5mg dochicin visa. Epicardial ablation has been shown to enhance outcome and must be considered in these instances antimicrobial gym bag for men order dochicin, maybe as the preliminary ablation technique virusbarrier 0.5mg dochicin overnight delivery. Early implantation of main prevention implantable cardioverter defibrillators for sufferers with newly diagnosed extreme nonischemic cardiomyopathy infection esbl generic 0.5mg dochicin otc. Utility of the wearable cardioverter-defibrillator in sufferers with newly diagnosed cardiomyopathy a decade-long single-center expertise. Outcomes of catheter ablation of ventricular tachycardia within the setting of structural heart disease. Early referral for ablation of scar-related ventricular tachycardia is related to improved acute and long-term outcomes: results from the center middle of Leipzig ventricular tachycardia registry. Outcome of ventricular tachycardia ablation in sufferers with nonischemic cardiomyopathy: the impact of noninducibility. Long-term consequence after catheter ablation of ventricular tachycardia in sufferers with nonischemic dilated cardiomyopathy. Isolated septal substrate for ventricular tachycardia in nonischemic dilated cardiomyopathy: incidence, characterization, and implications. Clinical influence of mapping strategies for treatment of ventricular tachycardias in sufferers with structural heart disease. Mapping of a postinfarction left ventricular aneurysm-dependent macroreentrant ventricular tachycardia. Regional myocardial wall thinning at multidetector computed tomography correlates to arrhythmogenic substrate in postinfarction ventricular tachycardia: assessment of structural and electrical substrate. The have to modify affected person choice to improve the benefits of implantable cardioverter-defibrillator for major prevention of sudden demise in non-ischaemic dilated cardiomyopathy. Primary prevention of sudden cardiac demise in a nonischemic dilated cardiomyopathy population reappraisal of the function of programmed ventricular stimulation. Multiple autonomic and repolarization investigation of sudden cardiac death in dilated cardiomyopathy and controls. Myocardial scar predicts monomorphic ventricular tachycardia but not polymorphic ventricular tachycardia or ventricular fibrillation in nonischemic dilated cardiomyopathy. Impact of the presence and amount of myocardial fibrosis by cardiac magnetic resonance on arrhythmic outcome and sudden cardiac dying in nonischemic dilated cardiomyopathy. Late gadolinium enhancement and the danger for ventricular arrhythmias or sudden death in dilated cardiomyopathy. Survival after secondary prevention implantable cardioverter-defibrillator placement. Absolute danger discount in total mortality with implantable cardioverter defibrillators: analysis of major and secondary prevention trial information to assist risk/benefit evaluation. Implantable cardioverter defibrillators for main prevention of mortality in sufferers with nonischemic 22. Percutaneous left ventricular assist gadgets in ventricular tachycardia ablation multicenter expertise. Characteristics of intramural scar in sufferers with nonischemic cardiomyopathy and relation to intramural ventricular arrhythmias. Combined endocardial and epicardial catheter ablation in arrhythmogenic right ventricular dysplasia incorporating scar dechanneling method. Endocardial unipolar voltage mapping to detect epicardial ventricular tachycardia substrate in sufferers with nonischemic left ventricular cardiomyopathy. Infarct transmurality as a criterion for first-line endo-epicardial substrate-guided ventricular tachycardia ablation in ischemic cardiomyopathy. Characteristics of medical and induced ventricular tachycardia throughout a quantity of ablation procedures. Endocardial ablation to eliminate epicardial arrhythmia substrate in scar-related ventricular tachycardia. Scar homogenization versus limited-substrate ablation in sufferers with nonischemic cardiomyopathy and ventricular tachycardia. Recent advances in ablation of ventricular tachycardia associated with structural heart illness. Catheter ablation of ventricular tachycardia and mortality in patients with nonischemic dilated cardiomyopathy: can noninducibility after ablation be a predictor for decreased mortality
The transverse portion of the cruciform ligament is often referred to as the transverse ligament antibiotic drops for swimmer's ear buy dochicin 0.5mg. The transverse ligament is attached to the tubercles on the medial aspect of every lateral mass of the atlas and is important in maintaining atlantoaxial stability bacteria vs bacterium order dochicin in india. Positioned anterior to the transverse ligament antibiotic impregnated cement generic dochicin 0.5 mg fast delivery, the apical ligament extends from the tip of the dens to the basion antibiotic use in livestock buy dochicin once a day. The paired alar ligaments connect the lateral aspect of the odontoid to the medial facet of the occipital condyles and limit lateral bending forces as well as rotational forces. Barring vertebral artery anomalies, the paired arteries lengthen by way of the transversarium at the stage of the axis and right into a transverse groove above the superior articular aspect of the atlas. Due to their proximity, the vertebral arteries, inner carotid vasculature, and cranial nerves are all weak to injury and require particular attention during examination. The distinctive anatomical relationships within this osseoligamentous advanced account for the injury patterns seen in the occipitoatlantoaxial spine. Unrecognized trauma to the upper cervical backbone can end result in devastating outcomes with harm to the brainstem and spinal twine. Nowadays, regularly bettering resuscitation protocols and lifesaving measures have increased the incidence of sufferers surviving high-energy trauma with concomitant atlantoaxial injury. Radiographs and advanced imaging methods are utilized to assist surgeons in prognosis and treatment planning. In this text, the authors discuss the prognosis, anatomy, clinical evaluation, and surgical stabilization techniques for traumatic atlantoaxial subluxation. The focus of this chapter is on the traumatic causes of atlantoaxial subluxation and their respective administration. Traumatic atlantoaxial instability is notably seen in a bimodal distribution in youthful sufferers as 66 Management of Traumatic Atlantoaxial Subluxations eight. In the setting of higher cervical backbone harm, diaphragm and intercostal musculature may paralyze and lead to respiratory failure. The remainder of the backbone should also be evaluated as noncontiguous backbone injuries are as excessive as 6% in trauma sufferers. Posterior scalp sensation within the distribution of the larger occipital nerve could additionally be diminished and cranial nerve injury is feasible. Vaccaro et al demonstrated a 20% danger of vertebral artery harm in nonpenetrating cervical backbone trauma. They account for an estimated 10% of all cervical spine fractures and 25% of accidents to the atlantoaxial advanced. Half of patients with atlas fractures have one or more other cervical backbone fractures and 40% are associated with fractures of the axis. Treatment normally consists of soft cervical collar immobilization for a quick while since it is a steady injury. This damage kind produces bilateral anterior and posterior arch fractures and will cause C1�C2 instability relying on the integrity of the transverse ligament. In the setting of instability, C1�C2 or occiput�C2 fusion may be required for maintenance of neurological status and initiating early rehabilitation. Flexion-extension views are omitted due to danger of progressive neurological harm within the setting of instability as well as affected person guarding. Sagittal steadiness is maintained within the cervical spine when lines drawn between the anterior border of the vertebral bodies, posterior border of the vertebral bodies, anterior aspect of the lamina, and spinous processes, are all continuous. Instability and potential spinal wire compression are assessed on the premise of following measurements: 1. On the opposite hand, if it stays unstable with C1�C2 translation after 2 to three months of immobilization, then surgery could be proposed and would be both a C1�C2 or an occiput�C2 fusion. The ranges of the fusion would depend on the local bony anatomy, the diploma of malalignment of the occipitocervical joint, and the placement and patency of the vertebral arteries. It must be emphasised that drilling, tapping, and screw insertion into the atlas lateral lots may be extremely challenging and may not be possible if the atlas lateral masses are completely loose and independently cell. Lateral mass fractures with greater than 5 mm of displacement must be immobilized using a inflexible cervical collar or hardly ever utilizing a inflexible occipito-cervical-thoracic brace. Minimal or nondisplaced injuries ought to be treated definitively with inflexible cervical collar immobilization for six weeks. Of the 23 sufferers with greater than 1-year follow-up, 57% reported vital symptoms including neck pain, scalp dysesthesias, and/or neck stiffness. The injury has brought on an avulsion of the bony origin of the transverse ligament from the proper lateral mass of C1 (arrow).
Very early diastolic potentials (in the first half of diastole) can represent an space of slow conduction at the entrance of a protected isthmus antimicrobial herbs and spices discount 0.5 mg dochicin with mastercard. These potentials stay fixed to the prior tachycardia complicated (exit web site from the isthmus) virus kills kid purchase genuine dochicin, and a delay between this complicated and the next tachycardia complex would mirror a delay in coming into or propagating via the protected diastolic pathway infection of the colon purchase cheap dochicin. This reentrant circuit has a number of components-a widespread pathway antibiotic resistance animation ks4 purchase 0.5mg dochicin mastercard, an exit website, an outer loop, an internal loop, an entry website, and bystander websites. Because this zone of gradual conduction is usually composed of a small quantity of myocardium and is bordered by anatomical or useful obstacles stopping the spread of the electrical sign except in the orthodromic direction, propagation of the wavefront in the protected isthmus is electrocardiographically silent. The reentrant wavefront propagates by way of the outer loop while on the same time activating the the rest of the myocardium. The inner loop can serve as an integral part of the reentrant circuit or function as a bystander pathway; the timing of activation, just like the outer loop, is usually throughout electrical systole. An connected bystander website represents a dead-end pathway (or a blind pouch) that communicates with the common central pathway or any internal loop and has no different exits. When a premature stimulus is delivered to websites distant from the reentrant circuit, it could interact with the circuit in several methods. When the stimulus is late-coupled, it may reach the circuit after it has just been activated by the reentrant wavefront. Consequently, though the extrastimulus may have resulted in activation of part of the myocardium, it fails to have an effect on the reentrant circuit, and the reentrant wavefront continues to propagate within the important isthmus and thru the exit web site to produce the subsequent tachycardia complex on time. To reset a reentrant tachycardia, the paced wavefront must attain the reentrant circuit (entry site), encounter excitable tissue throughout the circuit. Time-consuming, point-by-point maneuvering of the catheter is required to hint the origin of an arrhythmic event and its activation sequence in the neighboring areas. The success of roving point mapping is dependent upon the sequential beat-by-beat stability of the activation sequence being mapped and the power of the patient to tolerate sustained arrhythmia. Therefore it may be difficult to perform activation mapping in poorly inducible tachycardias, in hemodynamically unstable tachycardias, and in tachycardias with unstable morphology. Sometimes poorly tolerated fast tachycardias may be slowed by antiarrhythmic agents to allow for mapping. Alternatively, mapping can be facilitated by starting and stopping the tachycardia after data acquisition at each web site. Moreover, the laborious means of precise mapping with standard strategies can expose the electrophysiologist, workers, and patient to undesirable ranges of radiation from the extended fluoroscopy time. The lack of ability to accurately associate the intracardiac electrogram with a particular endocardial site accurately also limits the reliability with which the roving catheter tip may be placed at a site that was beforehand mapped. This leads to limitations when the creation of lengthy linear ablation lesions is required to modify the substrate, in addition to when multiple isthmuses or channels are current. The inability to determine, for instance, the positioning of a previous ablation increases the danger of repeated ablation of areas already dealt with and the likelihood that new sites can be missed. The illustration exhibits a standard diastolic pathway, entrance and exit sites, inner and outer loops, adjoining bystander dead-end paths in three places, and distant bystander websites. If the extrastimulus encounters absolutely excitable tissue, as generally happens in reentrant tachycardias with massive excitable gaps, the tachycardia is advanced by the extent that the paced wavefront arrives on the entrance web site prematurely. If the tissue is partially excitable, as can occur in reentrant tachycardias with small or partially excitable gaps, and even in circuits with large excitable gaps when the extrastimulus could be very untimely, the paced wavefront will encounter some conduction delay within the orthodromic course inside the circuit. Therefore the reset tachycardia complex may be early, on time, or later than anticipated. In the retrograde course, it encounters increasingly recovered tissue and is ready to propagate till it meets the incoming circulating wavefront and terminates the arrhythmia. However, following the first stimulus of the pacing prepare that penetrates and resets the reentrant circuit, the next stimuli work together with the "reset circuit," which has an abbreviated excitable hole. The first entrained complicated results in retrograde collision between the stimulated and the tachycardia wavefronts, whereas in all subsequent beats, the collision happens between the presently stimulated wavefront and that stimulated previously. Depending on the diploma that the excitable hole is preexcited (shortened) by the primary resetting stimulus, subsequent stimuli can fall on absolutely or partially excitable tissue.
Upright open-mouth odontoid (d) and lateral (e) plain radiographs present passable cervical alignment infection prevention week discount 0.5mg dochicin visa. After consultation with endovascular neurosurgeon antibiotic 9 fk unsri discount dochicin 0.5 mg online, he was treated conservatively with exhausting cervical collar immobilization and every day aspirin for his vertebral artery occlusion treatment for dogs back legs buy dochicin once a day. A plough fracture is an unstable anterior arch fracture due to antibiotics for uti liquid order dochicin line the posterior shear force that causes the dens to plough by way of the anterior atlas, inflicting a posterior atlantoaxial dislocation. His research utilized cadaveric specimens and the findings had been confirmed by Fielding et al. The authors concluded that type I accidents are inherently unstable and unlikely to heal with out inside fixation. All of the available evidence is predicated on case series, retrospective reviews, and expert opinions. A steady harm might be handled with cervical collar immobilization for 6 to 12 weeks. He refused treatment, including onerous cervical collar, and introduced 4 weeks later to the emergency department complaining of severe neck pain and arm paresthesia. At three months follow-up, his paresthesia resolved and his neck improved significantly; upright lateral (g) and anteroposterior (h) radiographs present preserved cervical alignment. In a sequence of 29 patients with nondisplaced atlas fracture, therapy with halo vest resulted in 96% therapeutic. Treatment choices include inflexible cervical immobilization, cervicothoracic brace, halo vest, posterior fusion, and osteosynthesis (anterior or posterior). Osteosynthesis sounds interesting in concept, as bony reduction is achieved, and no fusion is important. Some consultants suggest initial traction to scale back the fracture, adopted by 12 weeks of halo vest immobilization. Atlantoaxial stability is then assessed with flexion-extension radiographs, and if instability continues to be current, then C1�C2 instrumented fusion is recommended. However, a comminuted atlas lateral mass fracture might preclude enough screw purchase into C1. Occiput�C2 fusion could also be indicated for instances with displaced fractures, excessive comminution, subluxation, or when spinal twine or brainstem compression is current. Efforts should be taken to avoid extension of fusion to the occiput if attainable, because of the morbidity of fusing the entire craniocervical junction. Hadley et al evaluated 32 patients with atlas fractures; 5 of these had unstable Jefferson fractures. No sufferers developed indicators of instability or nonunion and none required subsequent surgical fixation. He suffered C1 anterior and posterior arch fractures (arrows), as well as T7�8 fracture with epidural hematoma and spinal wire compression, and underwent thoracic spine decompression and fusion. Initial management entails placement in rigid cervical immobilization which is enough for stable fractures similar to isolated posterior arch fractures, transverse process fractures, anterior tubercle fractures, and nondisplaced lateral mass fractures. Upright cervical spine radiograph with open-mouth odontoid views is beneficial in inferring the integrity of the transverse ligament. Even choose patients with burst fractures with higher than 7 mm of mixed displacement may be treated with halo vest for 12 weeks. Careful analysis of flexionextension radiographs should be accomplished following immobilization to rule out persistent atlantoaxial instability. C1�C2 posterior instrumented fusion could be carried out, with C1�C2 transarticular screws or C1 lateral mass screws and C2 pars/pedicle screws assemble as the preferred strategies. It is caused by partial or complete disruption of the posterior longitudinal ligament and tectorial membrane, in addition to the bilateral alar ligaments. Subluxation or dislocation may happen on the atlanto-occipital articulation, the atlantoaxial articulation, or each. Lateral plain radiographs have lower sensitivity but might pick up abnormal relationships among the basion, tip of the dens, and anterior atlas arch. Typically, the basion (the tip of the clivus) ought to point toward the tip of the dens. The prevalence of vascular injuries is excessive, including vertebral or carotid artery vasospasm, intimal tears, thrombosis, dissection, and pseudoaneurysm.
Buy 0.5 mg dochicin overnight delivery. Tea Tree Essential Oil Benefits.