
CLINICAL,FORENSIC,AND ETHICS CONSULTATION IN MENTAL HEALTH
Nasonex nasal spray
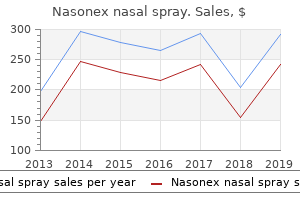
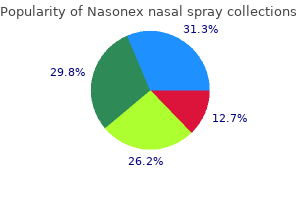
"Nasonex nasal spray 18gm for sale, allergy shots testing".
By: J. Pranck, M.B.A., M.D.
Co-Director, University of Texas at Tyler
However allergy testing east meadow purchase nasonex nasal spray 18 gm line, the 821 presentation can be more delayed into later childhood and maturity allergy forecast rockwall tx generic 18 gm nasonex nasal spray amex. This dysfunction also occurs as part of a syndrome together with Duchenne muscular dystrophy allergy shots made me worse buy nasonex nasal spray american express, glycerol kinase deficiency allergy shots depression order 18 gm nasonex nasal spray, and psychological retardation. Familial glucocorticoid deficiency is another form of inherited adrenal insufficiency. Hypoglycemia, seizures, and increased pigmentation are the presenting signs in such sufferers. Patients present with a number of congenital anomalies and typically with adrenal insufficiency. Autoimmune adrenalitis is the most common trigger (90% of the cases) of acquired adrenal insufficiency. The medulla is preserved whereas the cortex is markedly infiltrated with lymphocytes. The prognosis ought to be considered in patients with Addison disease of unknown etiology, and screening for very long�chain fatty acids is advisable. Tuberculosis was thought of a common cause of adrenal destruction however is much much less prevalent now. It can present as adrenal crisis and is referred to because the Waterhouse�Friderichsen syndrome. Adrenal hemorrhage in pediatrics can result in hypoadrenalism within the neonatal interval. These patients might current with an belly mass, anemia, unexplained jaundice, or scrotal hematoma. Medications, including rifampin and anticonvulsants (phenytoin, phenobarbital), induce steroid-metabolizing enzymes 822 (cytochrome P450 superfamily) in the liver and scale back the effectiveness and bioavailability of corticosteroid substitute therapy. It is used in the treatment of refractory Cushing syndrome and in the remedy of adrenal carcinoma. Children may present with anorexia, nausea, vomiting, diarrhea, and development failure. The typical distribution of hyperpigmentation is over the extensor surfaces of the extremities, notably in sunexposed areas. The mucous membranes (vaginal mucosa, gingival borders), axillae, and palmar creases are involved, and hyperpigmentation of these areas is the hallmark of Addison disease. In early infancy, the most common explanation for adrenal insufficiency is sepsis, inborn errors of steroid biosynthesis, adrenal hypoplasia congenita, and adrenal hemorrhage. Laboratory Findings Hypoglycemia, hyponatremia, hyperkalemia, and ketosis are widespread. The affected person is considered to have a standard response if the 60-minute cortisol measures 18 g/dL. Stress doses of hydrocortisone, ideally a water-soluble type, similar to hydrocortisone sodium succinate, ought to be given intravenously. Acute doses of 10 mg for infants, 25 mg for toddlers, 50 mg for older kids, and one hundred mg for adolescents ought to be administered immediately and then each 6 hours for the first 24 hours. These doses may be tapered during the subsequent 24 hours if the patient has a passable progress. Most of the sufferers require persistent substitute remedy for his or her cortisol and aldosterone deficiencies. Hydrocortisone could also be given orally in doses of 10 mg/m2/day in three divided doses. During stress, corresponding to infection or minor operative procedures, the dose of hydrocortisone should be increased two- to threefold. If aldosterone deficiency is current, fludrocortisone (Florinef), a mineralocorticoid, is given orally in doses of zero. These precursors have some mineralocorticoid activity, which compensate partially for the aldosterone deficiency. Thus, partial salt loss is the similar old presentation somewhat than the typical salt-losing crisis of full mineralocorticoid deficiency. The infant presents with dehydration, hyponatremia, and hyperkalemia despite marked elevation of aldosterone and renin levels.
Cyclophosphamide allergy treatment under tongue purchase generic nasonex nasal spray pills, ifosfamide allergy shots while on antibiotics buy nasonex nasal spray without prescription, methotrexate allergy medicine 999 buy nasonex nasal spray on line amex, and doxorubicin are identified to trigger hemorrhagic cystitis and mucositis allergy medicine while breastfeeding order cheap nasonex nasal spray. Hemorrhage in most cancers sufferers may result from defective hepatic clotting issue synthesis or hyperfibrinolysis. Patients can have decreased vitamin K availability or absorption with extended antibiotic use, poor oral consumption, or diarrhea. Other risk components embody chemotherapy, radiation, surgery, major tumor type/size, the presence of metastatic disease, obesity, immobility, complete parenteral diet, 922 and inherited thrombophilia. Other agents related to thrombotic occasions include vincristine, the anthracyclines, and prednisone. Thrombolysis is considered in selected cases and is associated with a major danger of bleeding. Precipitation of the urate or calcium phosphate crystals in the renal tubules might lead to renal failure. Uric acid control may be achieved with recombinant urate oxidase (rasburicase) or with a xanthine oxidase inhibitor (allopurinol). Severe hyperkalemia should be treated with insulin, glucose, bicarbonate, calcium, -adrenergic brokers (hyperventilation to induce alkalosis can be used acutely), potassium exchange resins, and renal substitute remedy. The lowest calcium dose required to relieve hypocalcemic symptoms should be used because of the risk of calcium phosphate precipitation. Hyperphosphatemia is managed with oral phosphate binders, such as sevelamer hydrochloride, or aluminum hydroxide. The epidural space is the most common area for spinal twine metastasis with the thoracic backbone being the most common website. Common signs embrace sensory abnormalities (40%�90%), focal weakness (75%), and bowel and bladder dysfunction (40%�50%). Craniospinal T1- and T2-weighted magnetic resonance imaging is the research of option to demonstrate epidural involvement, intraparenchymal unfold, or compression of nerve roots. Therapy (usually corticosteroids) should be initiated as soon because the prognosis is considered. Patients with posterior mediastinal lots are 923 in danger for spinal twine compression. Lesions affecting the tracheobronchial tree may trigger dyspnea, orthopnea, stridor, cough, and respiratory distress. Tumor plenty compressing the great vessels could cause head and neck edema with or with out neurological deficit. Supine place or sedation may worsen signs or lead to cardiopulmonary arrest, so careful planning of analysis and administration is necessary. Airway instrumentation must be carried out in a controlled surroundings by experienced anesthesiologists with surgical and cardiopulmonary help available when attainable. In most situations, endotracheal intubation takes place in acutely aware and spontaneously breathing patients employing topical anesthetic strategies with gentle sedation and avoiding neuromuscular blocking brokers. Reinforced endotracheal tubes of decreased diameter but sufficient length to prolong past the compression may be needed. Extracorporeal membrane oxygenation or cardiopulmonary bypass back-up should be thought of. Prebiopsy cytoreductive remedy utilizing corticosteroids or radiation may be required in patients presenting with severe airway compromise (may scale back the ability to make a definitive diagnosis). Progressive venous congestion and airway compression usually cause facial engorgement, headache, plethora, cyanotic facies, cough, dyspnea, orthopnea, hoarseness, stridor, and dysphasia with or with out pleural and/or pericardial effusions. Once the definitive diagnosis is reached, the appropriate chemotherapeutic plan will scale back tumor load quickly with enchancment of signs. Thrombolytic remedy must be considered in sufferers with in depth thromboembolism if no contraindications. Other infections to be thought of embody invasive fungi (mucormycosis), bacterial necrotizing pneumonias because of Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella, and tuberculosis. Noninfectious etiologies include main endobronchial tumors, diffuse alveolar hemorrhage, bronchiectasis, and international our bodies. The halo sign, a dense nodular lesion surrounded by ground glass attenuation (>180�), may be seen. Aggressive remedy of related coagulopathy, thrombocytopenia, and anemia and acceptable antibiotics or antifungals are warranted. Bronchoscopy should be considered if endoluminal management of the bleeding is feasible.
Buy 18gm nasonex nasal spray with amex. Causes Symptoms and Treatment of Drug allergy.

Diastolic dysfunction develops early and once overt systolic failure ensues allergy forecast baton rouge generic nasonex nasal spray 18gm mastercard, survival is poor allergy symptoms to mold purchase nasonex nasal spray 18gm amex, and consideration should be given to retransplantation allergy treatment urdu cheap nasonex nasal spray 18gm with amex. Patients with syncope should receive an automated implantable cardioverter defibrillator allergy testing on your back buy nasonex nasal spray us. Percutaneous coronary interventions might have a task in select sufferers but are restricted by the diffuse and small-vessel nature of the disease. Early outcomes for late retransplantation (more than 6 months after primary transplant) are much like those for major transplantation. Infections Infection is second to graft failure as a reason for death within the first 30 days and through the remainder of the first 12 months. Therapy contains discount of immunosuppression and the administration of antiviral brokers (without proven benefit), monoclonal antibodies in opposition to B-cell antigens (rituximab), chemotherapy, and cellular (adoptive) immunotherapy. Progressive renal dysfunction because of calcineurin inhibitor toxicity is increasingly problematic in long-term survivors (leading to renal transplantation). The enchancment in survival over the previous couple of years is due to reduction in early mortality. Oneyear survival is ~90%, with a comparatively small drop over the following 3�4 years. Disorders of surfactant protein synthesis may lead to end-stage lung disease also prompting referral for lung transplantation. Evaluation and Care of the Transplant Candidate Careful selection and timing are important to optimize outcomes. Patients are offered at a multidisciplinary conference such that laboratory testing, pulmonary function, and anatomic considerations can be taken into account. Nutritional standing ought to be optimized, intercurrent infections prevented, and muscle mass maintained with common train. Intubating a patient with impending respiratory failure secondary to end-stage lung illness, notably those who have been maintained on noninvasive assist, may be difficult. Prolonged desaturation and compromised cardiac output immediately following the procedure should be anticipated. Following intubation, patients with obstructive lung disease should be positioned on ventilator settings that can permit for a chronic expiratory section. Deep sedation and, frequently, neuromuscular blockade are required to facilitate interaction with the ventilator. Extracorporeal Support as Bridge to Lung Transplantation Recent advances in devices and methods have led to enhancements in outcome. The capacity to awaken and extubate these sufferers helps to minimize issues associated to long-term ventilation and sedation (infection, muscle fatigue, and organ dysfunction). Other gadgets have been used, such as a membrane oxygenator with cannulation of the pulmonary artery and left atrium. Postoperative Management and Early Complications Acute Complications 534 Reperfusion Injury/Graft Failure. Reperfusion harm happens from restoring blood provide to the ischemic donor lungs throughout and after transplant. Acute rejection can current with poor fuel trade, growing chest tube drainage, frothy sputum, and worsening fuel exchange. Pathologically, acute rejection is seen as infiltrates within the perivascular and interstitial regions with associated airway inflammation. Recurrent rejection warrants consideration of change within the immunosuppression routine. Varying degrees of systemic inflammatory response occur in the quick posttransplant interval. Postoperative bleeding is widespread and arises from vascular anastomoses, surgical planes of dissection, or airways. Bleeding threat is related to preoperative an infection, duration of surgery, and organ function. Phrenic nerve injury is frequent particularly after bilateral lung transplantation and can complicate postoperative respiratory restoration. Posttransplant Surveillance: Bronchoscopy, Computerized Tomography, Radiographs, Pulmonary Function Testing Daily chest radiographs are routine while chest tubes are in place and are used to follow lung parenchymal changes, assess lung volumes, examine catheter and tube position, and to detect evolving effusions. Bronchoscopy is carried out at 24 hours posttransplant to examine mucosal and anastomotic integrity and graft perfusion, and to clear bronchial secretions/blood.
Late acute rejection episodes (after the first year) carry a poor long-term prognosis allergy testing nashville nasonex nasal spray 18gm overnight delivery, especially if associated with graft dysfunction allergy symptoms headache nausea dizziness order nasonex nasal spray without a prescription. Unless there are particular contraindications allergy medicine ingredients order nasonex nasal spray 18 gm free shipping, full hemodynamic support allergy treatment under the tongue buy 18 gm nasonex nasal spray fast delivery, together with mechanical support, should be used because the situation is commonly reversible. Chronic Rejection and Posttransplant Coronary Arterial Disease the phrases chronic rejection and posttransplant coronary arterial illness are typically used synonymously. Coronary disease subsequent to transplantation is an accelerated vasculopathy and the leading cause of demise among late survivors. Use of older donors, donor cigarette utilization, late acute rejection episodes, older recipient age, retransplantation, and black race are a few of the threat factors reported for the development of posttransplant coronary arterial disease. Symptoms of ischemia are sometimes absent, although some kids expertise episodes of abdominal pain and/or chest pain regardless of operative denervation of the heart. Syncope and sudden demise are also widespread presentations of graft coronary disease in youngsters. In the current era, the analysis is most frequently made throughout surveillance-selective coronary angiography. Subacute Complications Airway dehiscence was a typical complication avoided by means of donor and recipient peribronchial tissue approximated close to the anastomotic web site to restore some bronchial circulation. Bronchial stenosis can have an result on 10% of circumstances and may be handled with bronchoscopic dilation. Cardiovascular Considerations Inotropic Agents and Cardiopulmonary Interactions the instant posttransplant lung recipient is on pressors. Dysrhythmias Atrial flutter or fibrillation is reported in practically 10% of circumstances and thought to be generated by electrical aberrance from the suture lines for pulmonary venous anastomosis. Systemic Hypertension Hypertension is common due to high-dose steroids, calcineurin inhibitors, or acute kidney dysfunction (from cardiopulmonary bypass or nephrotoxic medications). Respiratory Support Control of Ventilation Lung transplant recipients can have deep (hyperpnic) and infrequent (hypopneic) breaths due to the denervated donor organs. It might lead to patient�ventilator dyssynchrony, vital discomfort, and agitation. Criteria for Extubation Early extubation permits weaning of sedatives and facilitates pulmonary rest room. Adequate fuel trade, good mucosal perfusion and integrity, and hemodynamic stability are the standards. Gastrointestinal Complications Gastrointestinal issues are frequent, especially gastroesophageal reflux disease and postoperative ileus. Endocrine Considerations Hyperglycemia could end result from pancreatic insufficiency in cystic fibrosis sufferers or from a high-dose steroid immunosuppressive routine. Infectious Precautions Lung transplant recipients are more vulnerable than different solid-organ recipients to infections because of colonization of recipient and donor airways. Infections delay restoration, have an effect on transplanted and different organ capabilities, hamper immunosuppression, and trigger morbidity and mortality. Cystic fibrosis sufferers have increased risk of infections and are particularly prone to infections from colonization with resistant organisms previous to transplant. Immunosuppression Current immunosuppressive regimens goal comparatively specific steps in the stimulation or activation of T cells or eliminating alloreactive B cells. Immunoprophylaxis Infectious complications account for more than 40% of deaths within the first 12 post-op months. Vaccinations must be administered as scheduled, vaccine response may be decreased, and live virus vaccines prevented. Outcomes Survival after pediatric lung transplantation is worse than any other solid-organ transplant (similar to adults). The reentrant circuit requires two distinct conducting pathways with gradual conduction in a single and unidirectional block within the other pathway. Reentrant arrhythmias have a daily fee with a sudden onset and termination; they can additionally be provoked by an electrical stimulus.